If you work with children, you know how amazing—and challenging—it can be to keep up with their dynamic development. Sometimes it seems like they’re growing in every direction at once. That’s why a holistic approach to psychological and educational evaluations is vital.
Yes, it’s useful to gather single-domain data—such as pinpointing a clinical diagnosis or evaluating academic performance—but it’s so much more important to understand the whole child in context.
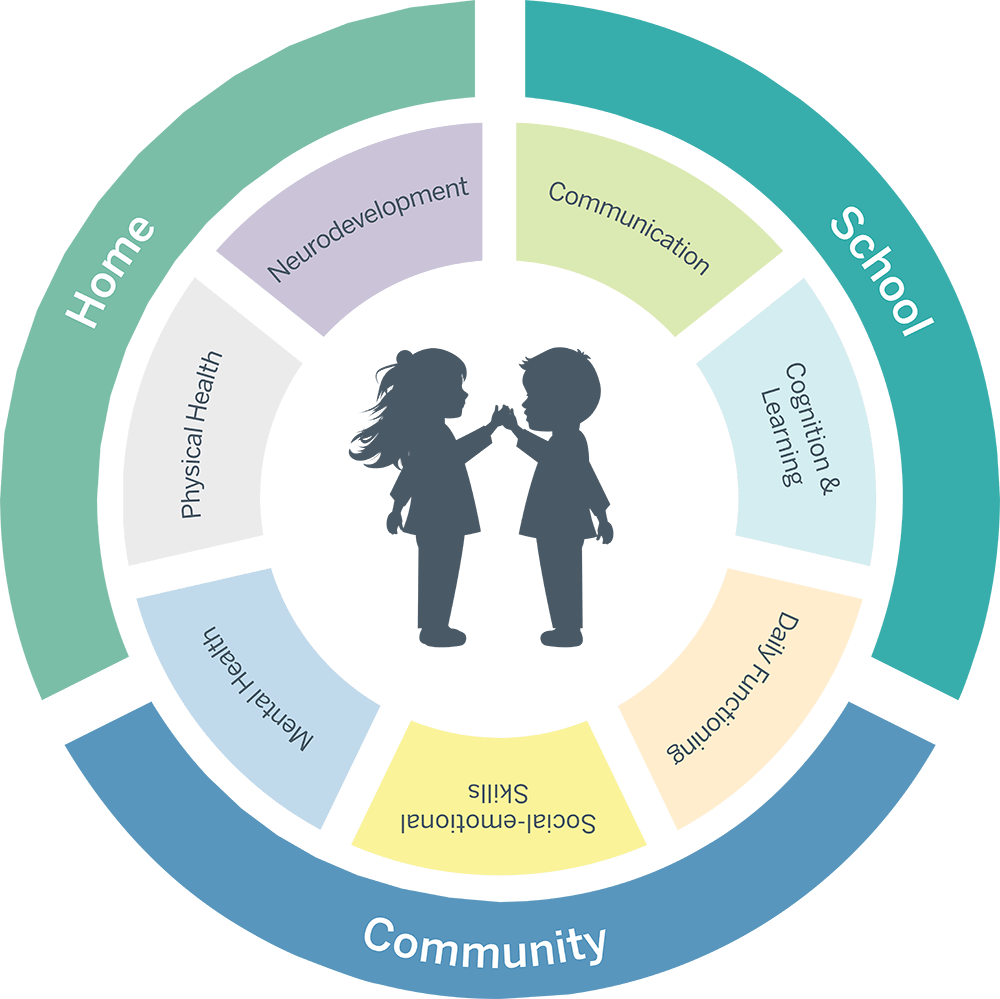
What is whole child assessment? It’s a strategy that integrates information about a child’s background, neurodevelopment, physical and emotional health, academics, daily functioning, and social relationships.
But…wait. Doesn’t a comprehensive strategy like that take more time? The short answer is yes. But on balance, a whole child approach likely saves time. Here’s why.
Siloed assessments address a single piece of complex puzzle. Holistic assessment, on the other hand, yields a more complete picture right from the start, so you and your team can design an instruction and intervention sequence that:
aligns with a child’s developmental trajectories;
prioritizes a child’s and family’s concerns;
follows the science of learning; and
sparks growth in multiple areas of a child’s life.
Because when it comes to a child’s development, every single day counts.
Early Development and the Whole Child
At no other time is the connection between brain and body clearer than it is during the early years of a child’s life. In the first year alone, nerves in the brain create about a million new connections every second. Those circuits extend throughout the nervous system, enabling a continuous flow of information from every system in the body.
During early development, the brain and body are continuously reading and responding to the environment. A child’s early experiences build the brain’s architecture, influencing developmental pathways and laying the groundwork for a lifetime of learning. Researchers have described the developmental process as “cumulative, progressive, intertwined, and cascading.” They say “critical cognitive, social, and emotional learning takes place as we learn to move and move to learn” (Stodden et al, 2023).
When you adopt a whole child approach to developmental assessment, you are studying a child’s sensory, motor, language, social, and emotional skills. You’re also gathering information about aspects of a child’s background that may have influenced development. And you’re using that information to plan intentional, sequential interventions that give a child access to a “physically active, cognitively engaging, and socially interactive” environment (Stodden et al., 2023).
It's a challenging endeavor! And WPS is happy to share the process with you, with tools that enable you to inform a whole child developmental strategy.
Whole child assessment aligns with the neuroscience of the brain-body connection.
Neuroplasticity—the brain’s ability to grow in response to new experiences—surges throughout the school years. Each new experience forms fresh neural pathways in the brain and body. These new circuits enable new functions.
Nutrition, sleep, social interactions, learning opportunities, sensory experiences, adversity, exposure to toxins, and so many other factors alter the structure and connectivity of the brain (Fandakova & Hartley, 2020). They enhance or inhibit the body’s growth and development. When you evaluate the whole child, you integrate these factors, so you can support health, well-being, and learning during periods of greater plasticity.
What does it do? Quickly identifies developmental strengths and weaknesses in five key areas: physical, social-emotional, adaptive behavior, cognitive, and communication; and offers suggested activities for intervention
How is it given? The examiner uses parent/caregiver interviews, parent/caregiver checklists, teacher checklists, and/or clinician rating scales.
How long does it take? 20–40 minutes
Who is it for? Children ages birth to 18; adults 18-21 years, 11 months
What does it do? Measures interpersonal engagement and understanding, including social responsiveness, joint attention, and symbolic comprehension
How is it given? The examiner systematically observes child activities
How long does it take? 15 minutes
Who is it for? Children ages 18 months to 4 years, 11 months
Neurodivergence and the Whole Child
As our understanding of neurodiversity grows, autism, attention-deficit/hyperactivity disorder (ADHD), and other neurodevelopmental conditions are increasingly recognized as whole child experiences. When health and education professionals conduct developmental screening of infants and toddlers, they track milestones across multiple domains including communication, emotion, social interaction, movement, and behavior.
When more in-depth evaluations are needed, experts recommend a comprehensive evaluation. That’s because neurodevelopmental conditions affect multiple aspects of identity, body systems, and areas of daily functioning in highly individual ways. A holistic assessment strategy allows practitioners to balance these tasks:
Identifying the unique constellation of features linked with a specific neurodevelopmental condition
Determining whether co-occurring conditions are present
Sequencing interventions to maximize benefits for families and children
Recommending further testing to explore related health effects
A comprehensive evaluation also looks at areas of development that aren’t necessarily part of the core characteristics of neurodevelopmental conditions.
Motor Skills
Neurodivergent children sometimes move differently than their neurotypical peers. In fact, motor delays are some of the earliest markers of autism. In addition, autism and ADHD frequently overlap with developmental coordination disorder. When children have trouble with motor control and coordination, they may not be able to explore their surroundings, play with their peers, or learn nonverbal communication methods as easily (Miller et al., 2024; Montes-Montes et al., 2021).
Sensory Processing
Neurodivergent children often process sensory information differently than their peers do. Some children with ADHD, for example, may experience “sensory overload” that leads to mental fatigue and difficulty with memory and attention. Researchers think these differences in sensory processing could even affect the way the brain develops (Fabio et al., 2024). Assessing sensory processing patterns can help you identify mismatches between a child’s sensory profile and their environmental conditions.
Executive Function
Executive function is a set of skills that helps people organize and plan so they can reach their goals. It includes working memory, the ability to shift our focus from one task to another, and the ability to exercise self-control. These skills are often associated with ADHD, but executive function differences are also common in autistic children. Research shows that executive function difficulties make it especially challenging for autistic children to use basic adaptive behaviors in school (Tschida & Yerys, 2022).
When you take a whole child approach to neurodevelopmental evaluations, you can explore strengths and needs across the specific domains you and your team feel are important for a child. You can collaborate with health and education professionals, family members, and neurodiverse children to plan the interventions that matter most right now. And you can re-design the environment so it’s a better fit for the whole child.
WPS invites you to explore these options as you build a comprehensive neurodevelopmental assessment plan.
Whole child assessment allows you to look for co-occurring conditions, contributing factors, and all possible explanations.
Mind and body are not separate entities. They are part of the same individual, each influencing the other. Together, they co-create the capabilities, personality, and life experience of the child.
When a child is showing signs of a health condition or learning difference, it’s vital to explore broadly. That’s because health conditions and learning differences don’t exist in isolation. They overlap. They interact with and influence each other, creating feedback and feed-forward loops that shape a child’s growth.
For example, autism and attention-deficit hyperactivity disorder (ADHD) involve similar genetic and neural features—but their neurocognitive profiles differ (Schachar et al., 2023). A holistic approach allows you to determine which characteristics and behaviors are likely to be related to which condition. Instruction, supports, and interventions can then be individually tailored and sequenced.
When you evaluate the whole child, you avoid reductive labels and one-dimensional intervention plans. Instead, you consider the entirety of a child’s lived experience.
What does it do? Identifies characteristics consistent with autism across developmental levels; provides information about a child’s characteristics to inform intervention and education plans
How is it given? Examiner observes and codes a child’s behavior in a playful, social encounter
What does it do? Identifies characteristics consistent with autism in children, teens, and adults; provides a comprehensive, strengths-based behavioral profile and guides family-friendly report-writing
How is it given? Examiner interviews parents, teachers, and individuals regarding language and communication, social relationships, emotional responses, sensory use, and interests
How long does it take? 30–90 minutes
Who is it for? Toddlers, children, teens, and adults
What does it do? Identifies characteristics consistent with autism; assists in distinguishing autism from other conditions
How is it given? Examiner interviews parents and caregivers about development and behavior in three functional domains: communication, social interactions, and interests
What does it do? Provides a complete picture of sensory integration and processing across multiple environments
How is it given? Parent/caregiver, school staff, and student complete rating scales describing the student’s visual, auditory, tactile, olfactory, gustatory, proprioceptive, and vestibular sensory experiences at home and school
How long does it take? 20–30 minutes for each of the 12 main forms; 10 minutes for each Environment Form
Who is it for? Children ages 4 months and older; adults to 87 years
What does it do? Evaluates executive function and self-regulation
How is it given? Parents, teachers, and adult individuals complete rating scales
How long does it take? 10 minutes; 5 minutes for screening version
Who is it for? Ages 5 to 18 years
Learning and the Whole Child
To be stunned by the end of a short story, awed by a cell on a microscope slide, or thrilled when your calculations turn out to be right—these are the joys we want for all students. Yet not every student experiences them. For some children, academics—and even the social dynamics at school—are an ongoing frustration.
Wherever and whenever students struggle, we look for solutions. It’s not enough to peruse scores on state tests. We need to understand why a student is having trouble—and what we can do about it. That’s why it’s so important to assess holistically. Because behind the numbers and letters and awkward interactions are children.
So, what should a holistic learning evaluation include?
The Centers for Disease Control and Prevention (CDC) has developed a Whole School, Whole Community, Whole Child (WSCC) framework to guide educators and health professionals working with students. Here’s what the CDC advises practitioners to consider:
Physical education and physical activity
Nutrition environment and services
Health education
Social and emotional climate
Physical environment
Health services
Counseling, psychological, and social services
Employee wellness
Community involvement
Family engagement
Dyslexia
Assessing dyslexia requires a comprehensive approach. It’s important to measure each of the skill areas recommended by the International Dyslexia Association. But it’s also important to consider the mental health effects of dyslexia, the possibility of overlapping neurodevelopmental conditions such as ADHD and autism, and the potential for a co-existing language disorder.
Motivation
Motivation isn’t a steadystate; for all of us, it rises and falls regularly. But a long-term drop in motivation can be an important clue to a learning difficulty, a shift in mental health, a change in a student’s environment, or a need for greater support (Cohen et al., 2022). Assessing student motivation can make it easier to understand a student’s experience and design supportive interventions.
Daily Functioning (Adaptive Behavior)
Adaptive behaviors are life skills that help us function day to day in different settings. We need to understand academic concepts, to interact with others appropriately, to handle money, to get back and forth to school or work, and to take care of ourselves physically and emotionally.
Measuring adaptive behaviors can help you understand whether a health condition, neurodevelopmental difference, or learning disability is affecting a child’s ability to cope with the demands of everyday life. Adaptive function assessments can also help you see if your interventions are improving a child’s overall functioning (Carpenter et al., 2022).
Whole child assessment enables you to consider each child in context, in community, and with continuity over time.
A child’s world can foster growth or limit it. That’s because each child’s environment contains both risk and resilience factors.
Beginning before birth, certain factors may make it more likely that a child will experience a health condition, developmental delay, or neurodevelopmental difference. A few of these factors are:
parental health
nutrition
illness or injury
birthplace
migration history
family income
learning opportunities
At the same time, a child’s family, culture, and community can be sources of strength through shared values, beliefs, capabilities, and systems of support.
When you work within a whole child framework, you can gather information about the child from parents, other educators, and clinicians who have firsthand knowledge of the child in varied settings. The Centers for Disease Control and Prevention (CDC) reports that when parents and school staff work together, student outcomes are better (CDC, 2019). A holistic approach also incorporates data gathered by a multidisciplinary team of professionals—leading to a more complete and actionable understanding of the child.
Considering the whole child in context allows you to prioritize the child’s and the family’s concerns and to design appropriate supports regardless of a specific diagnostic outcome (Rutherford et al., 2021). And you can keep track of a child’s response over time, so supports change as a child matures.
These assessments can help you create a holistic assessment strategy this year:
What does it do? Helps identify dyslexia and specific learning disability in reading, provides risk and probability indexes, and includes intervention recommendations based on assessment results
How is it given? Examiners can administer TOD-S to individuals or groups; TOD-C and TOD-E are individually administered; digital or paper formats
How long does it take? TOD-S: 10–15 minutes; TOD-E: additional 20–25 minutes after TOD-S; TOD-C: additional 30–40 minutes after TOD-S to obtain DDI, LPI, and RSI with additional tests at 5–10 minutes each
Who is it for? Children from grade K through adult; ages 5 years, 0 months–89 years, 11 months
What does it do? Measures early literacy skills, specifically phonological and print awareness, and allows examiners to easily track development using growth scores
How is it given? Examiner reads items from an easel stimulus book and the examinee provides nonverbal responses
How long does it take? 10–15 minutes
Who is it for? Children ages 3 years, 6 months to 8 years, 11 months
What does it do? Assesses comprehension of the concepts strongly related to early childhood cognitive and language development, school readiness, and early school achievement: colors, letters, numbers/counting, size/comparisons, shapes, and self/social awareness
How is it given? Examiner asks questions about basic concepts, and the child responds by pointing to text or pictures
How long does it take? 15–20 minutes
Who is it for? Children 3 years through 7 years, 11 months
That’s an expression educators and clinicians hear all too often. For the most part, it’s true. Children adapt to changing environments, marshal their resources, find creative workarounds, and rise to all sorts of challenges. Yet, a child’s resilience doesn’t erase the effects of coping with stress and adversity.
Toxic stress can change the brain’s structure, resulting in fewer neural connections in parts of the brain related to learning. When stress levels are too high for too long, brain chemicals and genes can also change, increasing the risk of later difficulties with mental health, behavior, and learning (de Magalhães-Barbosa, et al., 2022).
For a growing number of children and teens, toxic stress also leads to anxiety and depression disorders. These statistics may give you a sense of the scope of mental health difficulties in schools today:
About 5.8 million children in the U.S. have diagnosed anxiety disorders.
About 2.7 million have been diagnosed with a depression disorder (CDC, 2023).
42% of high school children said they felt hopeless for at least two weeks during the previous year (CDC, 2022).
When anxiety and depression walk you to school every day, it’s harder to concentrate in the classroom. Harder to remember instructions. Harder to be open to friendships. Anxiety and depression can also become “embodied,” leading to physical effects like these:
Sleep disturbance
Fatigue
Changes in appetite or weight
Substance use
Metabolic disorders (Morales-Muñoz et a., 2023)
Perhaps that’s why in 2022 the U.S. Preventive Services Task Force (USPSTF) recommended screening for anxiety in children and teens from ages 8 to 18 years. The USPSTF also recommended screening for major depressive disorder in teens from ages 12 to 18 years.
What makes a difference in a child’s resilience? Lots of factors, including good sleep, healthy nutrition, physical activity, and perhaps most important, the presence of warm and supportive grown-ups (Kahhalé et al., 2023). That’s where you come in. You may be able to notice signs of embodied stress, anxiety, or depression. You may be able to ask the important questions, conduct holistic assessments, and arrange the support a child needs.
Whole child assessment empowers you to leverage strengths and resilience factors.
Identifying diagnostic criteria is an important part of any evaluation. An accurate diagnosis can be liberating and can unlock the supports a child needs. But by necessity, diagnostic criteria tend to be deficit-based. Increasingly, practitioners are recognizing the need to design interventions and supports that build on assets, rather than simply addressing deficits.
For example, when researchers interview children with ADHD, students acknowledge their classroom struggles but also say they are optimistic, energetic, and capable of intense focus. They say their personal strengths and the involvement of their families helps them to be more resilient (Charabin et al., 2023). That’s just one example of the assets within and around a child. In your professional experience, you will certainly have seen many more.
When you adopt a whole child assessment practice, you can leverage a child’s interests and assets in your intervention plan. Researchers in one study noted, “When interventions are informed by a strengths-based perspective, they can work to improve the well-being and resilience of children by emphasizing or capitalizing on their strengths” (Charabin et al., 2023).
WPS offers a range of tools to help you evaluate the mental health and well-being of the students in your care.
What does it do? Measures cognitive, affective, and behavioral signs of depression
How is it given? Child examinee marks a list of behaviors and feelings focused on the core aspects of childhood depression; parents or caregivers complete rating scales
How long does it take? 5–15 minutes; 5–10 minutes for Short Form
Who is it for? Children and teens ages 7 to 17 years
What does it do? Measures psychological strengths and high-risk behaviors
How is it given? Parents, teachers, and individuals complete an inventory of psychological strengths and high-risk behaviors
How long does it take? 15–20 minutes
Who is it for? Ages 9 to 25 years
Language and the Whole Child
Communication is at the heart of human experience. At a very basic level, we communicate to survive. We also communicate to learn, build relationships, and engage in the activities that sustain us.
When clinicians and educators evaluate speech and language, they’re considering a child’s ability to process and comprehend what others are sharing, a skill known as receptive language. They’re also considering a child’s ability to communicate ideas, needs, and emotions, known as expressive language. Understanding a child’s speech and language gives us insight into so many other areas of a child’s experience.
In early development, language delays may be one of the first indicators of a neurodevelopmental difference such as autism or social communication disorder (Khan & Leventhal, 2023).
Delays in the early development of language are often intertwined with motor skill delays. The relationship between the two makes sense: Gestures, which are movements used with “communicative intentionality,” usually develop before spoken language skills emerge. In one study, researchers found that 1 in 2 young children with a communication disorder also had clinical or borderline scores on gross and fine motor skills (Varuzza et al., 2023).
Language difficulties can look like other conditions, such as dyslexia, autism, and behavioral issues. For example, a child who has trouble processing complicated verbal instructions may feel overwhelmed and frustrated, leading to disruptive behavior. While a behavioral episode may attract the attention of school leaders, addressing behavior without supporting the underlying language condition isn’t likely to improve outcomes for the child (Vermeij et al., 2021)
Language disorders can co-occur with neurodivergence, other health conditions, and learning disabilities (Schaeffer et al., 2023).
A close look at language abilities can help you distinguish between neurodevelopmental conditions that share some characteristics. For example, assessing pragmatic language may help you determine whether a child’s communication patterns are more consistent with autism or social communication disorder (ASHA, n.d.).
Language access is also a matter of equity and justice. Communicating with peers, teachers, and coaches is a big part of the day for most children. For children with language conditions, assistive technologies may allow them to participate more fully in their educational opportunities. The Individuals with Disabilities Education Act (IDEA) requires IEP teams to provide assistive devices and training where a child needs language access (IDEA, n.d.).
Whole child assessment moves us toward equity.
All children are entitled to a free and appropriate education. Yet disparities in educational outcomes and opportunities still exist for many children. Language barriers, social stigma, financial resources, and limited access to health services prevent some children from receiving the comprehensive evaluations they need.
When health and education professionals work with families and communities using a whole child approach, they can consider what additional supports and interventions are necessary to make success possible for everyone. We can “fulfill the vision that every child has access to supports that are developmentally and culturally appropriate” (Chafouleas & Iovino, 2021).
When we include language assessment in a holistic evaluation, we are also gaining valuable insights into other cognitive, emotional, and neurodevelopmental domains.
The ways people talk vary beautifully with regionality, accents, and cadence, but the importance of language itself is a constant. Language bridges mind, body, and environment—affecting just about every aspect of a child’s life experience.
WPS provides a full complement of speech and language assessments to help you capture the complex language needs of the children you serve.
What does it do? Provides a complete and integrated picture of oral and written language skills across a wide age range test
How is it given? Examiner presents a variety of oral and written language tasks; Examinee speaks, points, or writes their responses depending on the scale(s) administered
How long does it take? 10–20 minutes for Listening Comprehension Scale; 10–30 minutes for Oral Expression Scale; 10–30 minutes for Reading Comprehension Scale; 15–30 minutes for Written Expression Scale
Who is it for? Children ages 3 through 21 years for Listening Comprehension and Oral Expression Scales; 5 through 21 years for Reading Comprehension and Written Expression Scales
What does it do? Measures oral language processing skills, comprehension, and expression across four categories: Lexical/Semantic, Syntactic, Supralinguistic, and Pragmatic
How is it given? Examiner reads items aloud; examinee responds by speaking or pointing
How long does it take? 5–10 minutes for each test and 45 minutes for the General Language Ability Index
What does it do? Assesses listening comprehension—essential for classroom learning
How is it given? Examiner reads a passage and related questions aloud from a self-standing easel; Examinee responds orally—no reading or writing required
WPS Assessment Consultants are ready to help you design a holistic assessment strategy that meets the needs of your students, school, and community throughout the year.
WPS ProLearn™ offers professional development and training to support your team’s growth in whole child assessment.
Our Commitment to Your Holistic Practice
WPS has been supporting clinicians and educators in their quest to unlock human potential for over 75 years. We started with a single assessment to measure post-traumatic stress in veterans returning from overseas conflict. Today, we offer a full range of trusted, validated assessments so you can understand the lived experience of those in your care.
And WPS continues to invest in innovation. We’re working with researchers and experts to develop new assessments, design new administration options, and create new professional development opportunities to make your job easier and more effective.
Taking a whole child approach requires a team of professionals with excellent tools, experienced clinical judgment, and a desire to collaborate. WPS is proud to be part of your assessment team, and we look forward to sharing in your work this year.
Carpenter, K. L. H., Davis, N. O., Spanos, M., Sabatos-DeVito, M., Aiello, R., Baranek, G. T., Compton, S. N., Egger, H. L., Franz, L., Kim, S. J., King, B. H., Kolevzon, A., McDougle, C. J., Sanders, K., Veenstra-VanderWeele, J., Sikich, L., Kollins, S. H., & Dawson, G. (2022). Adaptive behavior in young autistic children: Associations with irritability and ADHD symptoms. Journal of Autism and Developmental Disorders, 10.1007/s10803-022-05753-2. Advance online publication. https://doi.org/10.1007/s10803-022-05753-2
Chafouleas, S. M., & Iovino, E. A. (2021). Engaging a whole child, school, and community lens in positive education to advance equity in schools. Frontiers in Psychology, 12, 758788. https://doi.org/10.3389/fpsyg.2021.758788
Charabin, E., Climie, E. A., Miller, C., Jelinkova, K., & Wilkins, J. (2023). "I'm Doing Okay": Strengths and resilience of children with and without ADHD. Journal of Attention Disorders, 27(9), 1009–1019. https://doi.org/10.1177/10870547231167512
Chen, M., & Mok, I. A. C. (2023). Perceived parental involvement influences students' academic buoyancy and adaptability: The mediating roles of goal orientations. Frontiers in Psychology, 14, 1248602. https://doi.org/10.3389/fpsyg.2023.1248602
Cohen, R., Katz, I., Aelterman, N., & Vansteenkiste, M. (2022). Understanding shifts in students’ academic motivation across a school year: the role of teachers’ motivating styles and need-based experiences. European Journal of Psychology of Education, 1–26. https://doi.org/10.1007/s10212-022-00635-8
de Magalhães-Barbosa, M. C., Prata-Barbosa, A., & da Cunha, A. J. L. A. (2022). Toxic stress, epigenetics and child development. Jornal de Pediatria, 98 Suppl 1(Suppl 1), S13–S18. https://doi.org/10.1016/j.jped.2021.09.007
Fabio, R. A., Orsino, C., Lecciso, F., Levante, A., & Suriano, R. (2024). Atypical sensory processing in adolescents with attention deficit hyperactivity disorder: A comparative study. Research in Developmental disabilities, 146, 104674. https://doi.org/10.1016/j.ridd.2024.104674
Fandakova, Y., & Hartley, C. A. (2020). Mechanisms of learning and plasticity in childhood and adolescence. Developmental Cognitive Neuroscience, 42, 100764. https://doi.org/10.1016/j.dcn.2020.100764
Goldberg H. (2022). Growing brains, nurturing minds: Neuroscience as an educational tool to support students' development as life-long learners. Brain Sciences, 12(12), 1622. https://doi.org/10.3390/brainsci12121622
Hancock, A., Northcott, S., Hobson, H., & Clarke, M. (2023). Speech, language and communication needs and mental health: The experiences of speech and language therapists and mental health professionals. International Journal of Language & Communication Disorders, 58(1), 52–66. https://doi.org/10.1111/1460-6984.12767
Kahhalé, I., Barry, K. R., & Hanson, J. L. (2023). Positive parenting moderates associations between childhood stress and corticolimbic structure. PNAS Nexus, 2(6), pgad145. https://doi.org/10.1093/pnasnexus/pgad145
Khan I, Leventhal BL. (2023, July 17). Developmental delay. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562231/
Miller, H. L., Licari, M. K., Bhat, A., Aziz-Zadeh, L. S., Van Damme, T., Fears, N. E., Cermak, S. A., & Tamplain, P. M. (2024). Motor problems in autism: Co-occurrence or feature?. Developmental Medicine and Child Neurology, 66(1), 16–22. https://doi.org/10.1111/dmcn.15674
Montes-Montes, R., Delgado-Lobete, L., & Rodríguez-Seoane, S. (2021). Developmental coordination disorder, motor performance, and daily participation in children with attention deficit and hyperactivity disorder. Children, 8(3), 187. https://doi.org/10.3390/children8030187
Morales-Muñoz, I., Mallikarjun, P. K., Chandan, J. S., Thayakaran, R., Upthegrove, R., & Marwaha, S. (2023). Impact of anxiety and depression across childhood and adolescence on adverse outcomes in young adulthood: A UK birth cohort study. The British Journal of Psychiatry, 222(5), 212–220. https://doi.org/10.1192/bjp.2023.23
Nygaard, M. A., Ormiston, H. E., Heck, O. C., Apgar, S., & Wood, M. (2023). Educator perspectives on mental health supports at the primary level. Early Childhood Education Journal, 51(5), 851–861. https://doi.org/10.1007/s10643-022-01346-x
Peterson, A., Charles, V., Yeung, D., & Coyle, K. (2021). The health equity framework: A science- and justice-based model for public health researchers and practitioners. Health Promotion Practice, 22(6), 741–746. https://doi.org/10.1177/1524839920950730
Rutherford, M., Maciver, D., Johnston, L., Prior, S., & Forsyth, K. (2021). Development of a pathway for multidisciplinary neurodevelopmental assessment and diagnosis in children and young people. Children, 8(11), 1033. https://doi.org/10.3390/children8111033
Schachar, R. J., Dupuis, A., Arnold, P. D., Anagnostou, E., Kelley, E., Georgiades, S., Nicolson, R., Townes, P., Burton, C. L., & Crosbie, J. (2023). Autism spectrum disorder and attention-deficit/hyperactivity disorder: Shared or unique neurocognitive profiles? Research on Child and Adolescent Psychopathology, 51(1), 17–31. https://doi.org/10.1007/s10802-022-00958-6
Schaeffer, J., Abd El-Raziq, M., Castroviejo, E., Durrleman, S., Ferré, S., Grama, I., Hendriks, P., Kissine, M., Manenti, M., Marinis, T., Meir, N., Novogrodsky, R., Perovic, A., Panzeri, F., Silleresi, S., Sukenik, N., Vicente, A., Zebib, R., Prévost, P., & Tuller, L. (2023). Language in autism: Domains, profiles, and co-occurring conditions. Journal of Neural Transmission, 130(3), 433–457. https://doi.org/10.1007/s00702-023-02592-y
Stodden, D. F., Pesce, C., Zarrett, N., Tomporowski, P., Ben-Soussan, T. D., Brian, A., Abrams, T. C., & Weist, M. D. (2023). Holistic functioning from a developmental perspective: A new synthesis with a focus on a multi-tiered system support structure. Clinical Child and Family Psychology Review, 26(2), 343–361. https://doi.org/10.1007/s10567-023-00428-5
Tschida, J. E., & Yerys, B. E. (2022). Real-world executive functioning for autistic children in school and home settings. Autism, 26(5), 1095–1107. https://doi.org/10.1177/13623613211041189
Varuzza, C., D'Aiello, B., Lazzaro, G., Quarin, F., De Rose, P., Bergonzini, P., Menghini, D., Marini, A., & Vicari, S. (2022). Gross, fine and visual-motor skills in children with language disorder, speech sound disorder and their combination. Brain Sciences, 13(1), 59. https://doi.org/10.3390/brainsci13010059
Vermeij, B. A. M., Wiefferink, C. H., Scholte, R. H. J., & Knoors, H. (2021). Language development and behavior problems in toddlers indicated to have a developmental language disorder. International Journal of Language & Communication Disorders, 56(6), 1249–1262. https://doi.org/10.1111/1460-6984.12665













![“There has been a tradition of single condition guidelines and pathways. [...] A singular focus on one presenting issue leads to the potential omission of other diagnoses (and supports). People may experience repetitive and lengthy assessment, a process which individuals and families find distressing and burdensome.” (Rutherford et al., 2021)](https://ecom-cdn.wpspublish.com/prod/media/wysiwyg/Research_brief-imagery/wctk-quote-2-min.png)











![“[I]f we care about providing environments that tend to the whole child, we also need to think about the whole teacher. We need to think about creating a system that supports the whole teacher and responds to their strengths, needs, and interests.” (McDonald, 2023) –Marisa Saunders, UCLA Center for Community Schooling Associate Director for Research](https://ecom-cdn.wpspublish.com/prod/media/wysiwyg/Research_brief-imagery/wctk-quote-5-min.png)